Arthritis
There are 2 main types of arthritis that affect the hip joint:
- Inflammatory arthritis:
This occurs when the body’s immune system attacks healthy tissues
including joints. Some types of inflammatory arthritis that can affect
the hip include rheumatoid arthritis, ankylosing spondylitis, and systemic
lupus erythematosus.
- Osteoarthritis (OA): this is a “wear
and tear” type of arthritis where the cartilage wears down until the
bones are touching – “bone on bone” – causing pain and stiffness of the
joint.
Cause
When arthritis is caused by DDH or FAI:
These
are conditions where the hip does not form properly during the growth
process in the womb or in childhood (Hip Dysplasia and Femoro-Acetabular
Impingement). There are treatments available for these conditions if
they are discovered in a baby or a child. When these conditions are not
discovered until adulthood, there is a high likelihood that
osteoarthritis will develop in the hip.
Symptoms
- Pain located in the groin or thigh, maybe radiating to the buttocks or the knee
- Pain may start slowly and gradually get worse
- Worse after sitting or resting for a prolonged period of time
- Can be painful at night while trying to sleep
- Stiffness in hip and may feel like it is locking or that it is giving way
- Decreased range of motion of the hip
- Limping
Diagnosis
Your
family doctor will discuss your history and symptoms with you, then
carry out a physical examination. An X-ray will be ordered to look at
your joint and to identify any bony changes.
Treatment
There is no cure for osteoarthritis.
Conservative treatments should be tried first to help relieve symptoms. These include:
- Education
- Rest and/or activity modification
- Weight loss
- Low impact exercise (swimming, aqua-fit, cycling)
- Use of a walking aid (cane, walker, walking poles)
- Use of NSAIDs (Advil/Ibuprofen) or pain relief medication (Tylenol/Acetaminophen)
- Physiotherapy and exercise
- Physiotherapy
should focus on promotion of physical activity and general health. The
physiotherapist will help you with pain control, hip mobility exercises,
hip, core and general strengthening exercises, assess your gait and
balance and possibly suggest a walking aid (e.g.: cane) if necessary.
The therapist will introduce non-weight-bearing exercise options such as
swimming, aqua-fit and cycling as well as a home exercise program
- Cortisone injection
- Cortisone
injections of the hip are performed using X-ray or ultrasound guidance
to ensure correct needle placement. These injections are generally done
in a hospital or by a sports medicine doctor in their office
Surgical treatment is indicated for patients with pain and loss of function despite a trial of conservative treatment.
Hip resurfacing or hip replacement are the two surgical options.
- Hip resurfacing
is generally only considered in patients who meet specific criteria. It
is contraindicated for women. Hip resurfacing involves placing a metal
cup in the acetabulum (socket) and then capping the femoral head (ball)
with a metal cap.
- Hip replacement is the most common
surgery to help with pain and loss of function in patients with severe
hip arthritis. It involves placing a metal cup that is lined with
ceramic or plastic in the acetabulum (socket). The femoral head (ball)
of the femur is removed and a metal rod is placed in the femur with a
ball portion of metal or ceramic.
Recovery time depends
on the procedure performed and the physical condition of the patient
prior to hip surgery. Physiotherapy is recommended after surgery. A typical
rehabilitation program will last 12 weeks.
Developmental Dysplasia (dislocation) of the Hip – DDH
In Developmental Dysplasia of the Hip (DDH), the socket (acetabulum) part of the hip joint is shallow, 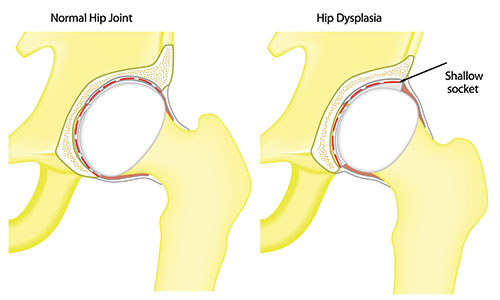 so that the ball (head of femur) portion does not fit into it properly. In childhood, this can make it easier for the hip to dislocate or for the ball to come out of the socket. The hip joint ligaments may also not be tight enough, which will make it easier for the hip to dislocate.
so that the ball (head of femur) portion does not fit into it properly. In childhood, this can make it easier for the hip to dislocate or for the ball to come out of the socket. The hip joint ligaments may also not be tight enough, which will make it easier for the hip to dislocate.
DDH tends to run in families and is more likely in females, first-born children, and babies born in the breech position.
Normally, this condition is diagnosed and treated in childhood. Sometimes the condition is not as obvious as a dislocation and it is not discovered until the person becomes an adult. The pain usually appears once the labrum becomes injured or torn.
Symptoms
In babies:
Some children will have no signs or symptoms until the toddler begins to walk, at which time an exaggerated waddling gait will be noticed. There could be a difference in leg length and possibly less mobility in one hip.
In adults:
- Hip pain and/or a limp are usually a first sign in a young adult. (Can be a painless limp.)
- Pain is felt deep in the groin, beginning intermittently but will increase with time
- Pain can be sharp and/or a dull ache
- Increasing pain with walking, standing and /or running
- Pain at night
- Sensation of hip catching, snapping, popping or locking that is painful
Diagnosis
In babies:
DDH in babies is diagnosed by a physical exam. A hip exam is routinely done to all babies in well-baby exam check-ups to screen for this condition. If DDH is suspected, the pediatrician will ask for an ultrasound at 6 weeks of age, followed by an X-ray at 4 months.
In adults:
Hip dysplasia is more of a challenge to diagnose in adults. Your doctor will listen to your history and symptoms, and will then carry out a physical exam. They may request an X-ray to have a better look at the joint.
Treatment
In babies:
If this condition is discovered in a baby, the doctors can use a special harness or braces to position and hold the baby’s hips in an optimal position to encourage normal hip joint development. If this does not work, hip surgery needs to be done to correct the condition. After surgery, a cast is worn to keep the hips aligned during healing.
In adults:
Surgical management is most often necessary to manage this condition once it is finally diagnosed in an adult. Hip preserving surgery (periacetabular osteotomy or hip arthroscopy) or hip replacement surgery are two surgical options. The choice of which type of surgery will depend on the state of your joint. Recovery times will depend on the type of hip surgery and your condition prior to surgery.
*see arthritis section for more information on hip replacement surgery
Conservative management is often helpful to delay hip surgery or to relieve pain until it is performed. Non-operative treatments are possible when the condition is caught early and there is minimal damage to the joint.
Conservative treatments include:
- Weight loss
- Heat/ice
- Activity modification (avoid running, stair climbing, impact sports)
- NSAIDs (Advil/Ibuprofen) or pain relief (Tylenol/Acetaminophen) medications
- Cortisone injection
- Cortisone injections of the hip are performed using X-ray or ultrasound guidance to ensure correct needle placement. These injections are generally done in a hospital or by a sports medicine doctor in his office.
- Low impact exercise (swimming, aqua-fit, cycling)
- Physiotherapy
- Physiotherapy treatment should focus on exercises to improve hip mobility, core and lower extremity strength, improve posture and general fitness, as well as make some suggestions of low/no impact activities such as swimming, aqua-fit, and cycling.
Femoro-acetabular Impingement - FAI
In Femoro-Acetabular Impingement (FAI), the anatomical shape of the ball and/or socket of the hip  joint can be mismatched because the bones/joint don’t quite develop properly during childhood. There can be a development of “bumps” or an over-deep socket. This deformity will cause abnormal contact between the ball and socket parts of the hip, leading to problems with range of motion of the hip. This can lead to tears in the labrum (the cartilage rim that lines the outside edge of your hip socket) and osteoarthritis (a thinning of the cartilage on the hip joint surfaces).
joint can be mismatched because the bones/joint don’t quite develop properly during childhood. There can be a development of “bumps” or an over-deep socket. This deformity will cause abnormal contact between the ball and socket parts of the hip, leading to problems with range of motion of the hip. This can lead to tears in the labrum (the cartilage rim that lines the outside edge of your hip socket) and osteoarthritis (a thinning of the cartilage on the hip joint surfaces).
There are 3 types of FAI:
Pincer, Cam and Combined – the classification depends on the location and type of deformity in the joint
Cause
Current thinking is that one can be predisposed to FAI by genetics or it is acquired because of repetitive activities/sports involving the hips at a younger age.
It most commonly affects those aged 30-45 years who have played sports regularly, or elite athletes and dancers in their teens or twenties.
Symptoms
FAI can be asymptomatic for some time. Common symptoms are:
- Sharp or pinching pain in groin area - can become a deep ache
- Worse after walking, walking up hill, or with prolonged sitting
- Worse with hip-twisting motion or squatting
- Catching, locking, clicking in the joint
- Limping
Diagnosis
Your doctor will discuss your history and symptoms with you and then carry out a physical examination. They will likely ask for hip X-rays to look at the bones in your joint. An MRI (possibly MRA) will be ordered if your doctor wants to look at the soft tissue in your joint because labral tears are quite common with FAI.
Treatment
Conservative treatment should be attempted first. These include:
- Rest and/or activity modification
- Weight-loss
- Low impact exercise (swimming, aqua-fit, cycling)
- Use of NSAIDs (Advil/Ibuprofen) or pain relief medications (Tylenol or Acetaminophen)
- Physiotherapy
- Physiotherapy treatment should focus on exercises to improve hip mobility, core and lower extremity strength, improve posture and general fitness, as well as make some suggestions of low/no impact activities such as swimming, aqua-fit and cycling.
- Cortisone injection
- Cortisone injections of the hip are performed using X-ray or ultrasound guidance to ensure correct needle placement. These injections are generally done in a hospital or by a sports medicine doctor in their office.
- A cortisone injection into the hip joint can help relieve pain but also be used as a way to diagnose your hip issue. Pain relief from the injection can prove that the pain is coming from inside your joint.
Surgical TreatmentSurgical treatment can be done with an arthroscopy of the hip. This involves small incisions where cameras and instruments are inserted into your hip and used to shave off the extra bone spurs in the joint and/or repair the damaged labrum (the cartilage rim that follows the outside edge of your hip socket). It can also be done as an open procedure.
In this LHIN region, the procedure is rarely done on anyone over the age of 40 or if the patient shows signs of arthritis in the hip joint.
Hip replacement surgery will be considered if conservative treatment is unsuccessful in managing the symptoms.
*see arthritis section for more information on hip replacement surgery
Hip labral tear
A labral tear involves the cartilage rim that follows the outside edge of your hip socket. The labrum deepens the socket and acts as a seal or gasket to help hold the ball securely in the socket.
Cause
Research shows that 75% of cases of torn acetabular labrum have no known direct cause.
The condition can be caused by:
- Trauma - a fall or sporting injury when the hip is forced into an extreme position
- Sporting activities involving extreme joint movement, contact or pivoting actions such as in hockey, soccer, football, golf, ballet and gymnastics
- Structural abnormalities such as Femoro-Acetabular Impingement (FAI) or Hip Dysplasia (DDH)
It is important to note that labral tears may represent a natural condition in an aging joint. Labral tears have been found in patients without hip pain. Their presence increases with age.
Labral tears may predispose you to developing hip arthritis in the future.
Symptoms
- Sharp, pinching pain in your groin that can become an ache.
- Pain can be felt deep in the joint, in the groin, over the side of the hip and/or deep in the buttock region
- Begin slowly and not necessarily related to a specific injury or will come on following an increase in activity or from an activity that you do not often do.
- Worse with activity but can progress to being felt while standing, walking and sitting (especially in tight spaces such as in the car, movie theatre or airplane)
- Catching, clicking and giving way of the hip
- Limping
- Rest does not always improve symptoms
Diagnosis
Labral tears are diagnosed by your history, symptoms and a physical examination where the doctor will look at specific hip movements and whether they reproduce your pain.
X-rays do not show a labral tear but may reveal the cause (FAI, DDH, trauma) and/or condition of your joint by identifying if you have signs of osteoarthritis. An MRI with dye (MRI arthrogram) is the most reliable test to confirm if you have a labral tear but is only done in specific circumstances.
Treatment
Conservative treatments include:
- Rest and/or activity modification
- Pain relief medication (Tylenol/Acetaminophen) and/or NSAIDs (Advil/Ibuprofen)
- Cortisone injection
- Cortisone injections of the hip are performed using X-ray or ultrasound guidance to ensure correct needle placement. These injections are generally done in a hospital or by a sports medicine doctor in their office.
- Physiotherapy
- Physiotherapy treatment can help with pain control, gait analysis, improving back and hip movement, strengthening the muscles around the hip, back and core as well as focus on function and fitness.
Surgical TreatmentHip surgery to repair labral tears is not usually done in patients over 40 and/or with signs of osteoarthritis as it often fails to relieve pain in these circumstances. According to recent research, it does not stop the progression of osteoarthritis and there is often the need to re-operate.
Osteonecrosis/Avascular Necrosis of the Hip - AVN
Thanks to blood circulation, the bone cells are constantly repairing themselves. Osteonecrosis/AVN occurs when the blood supply to the femoral head or ball portion of the hip becomes restricted or damaged. When this happens, it causes the bone structure to weaken, and collapse. This occurs especially on the part of the joint where most of the weight is concentrated, causing the ball portion of the joint to flatten, changing the shape of the ball and socket in the joint which leads osteoarthritis and pain in the hip.
AVN occurs more often in men aged 35-50 years old.
Causes
- Traumatic injury including breaking the hip
- Excessive alcohol use
- Smoking
- Blood clotting conditions and blood diseases (e.g.: Sickle cell anemia, leukemia)
- Long-term use of corticosteroid medications (e.g.: Prednisone)
- Some autoimmune conditions like Crohn’s or Lupus.
Diagnosis
Your doctor will discuss your history and symptoms, then carry out a physical examination. Your doctor will send you for an X-ray and possibly an MRI.
Symptoms
It may take from several months to years for the condition to progress.
- Dull ache or throbbing in the groin, buttocks and/or down the front of the thigh
- Begins slowly and does not seem to be caused by anything in particular
- Becomes difficult to stand or to walk over time
- Pain at rest
- Difficulty sleeping
Treatment
It is a slow-progressing disease, and the earlier it is diagnosed the better the outcome.
Awaiting hip surgery:
- Pain relief medication (Tylenol, Acetaminophen)
- Decreased weight-bearing on the affected leg
- Use of a walker or crutches
- Medications to treat bone loss (e.g.: Fosamax)
- Physiotherapy
- The physiotherapist will show you ways to stretch and strengthen your hip. Focus will be on keeping your hip mobile and flexible while protecting it.
There are a few procedures that are available to the surgeon to treat avascular necrosis but the two most common are:
Core decompression: The surgeon will drill one or more holes in the ball portion of your hip joint to create new blood vessels to the affected area and decrease the pressure that builds inside the bone. The surgeon may also choose to do a bone graft to stimulate bone growth. The bone tissue used for the graft is usually taken from the patient. This is all done through a very small incision in the side of the thigh with the help of a fluoroscope (a type of X-ray) to guide the surgeon. This is an outpatient procedure and you get to go home the same day.
Total hip replacement will be recommended for more advanced AVN as the condition is treated exactly the same as osteoarthritis of the hip.
*see arthritis section