Bunion (Hallux Valgus)/Bunionette
A bunion is a bony bump that develops on the inside of the foot at the big toe joint. Shifting of the bones may cause your big toe to move closer to the second toe. The bunion area may be red and swollen, and it may be painful to put on shoes and to walk. It may cause a callus to develop on the ball of the foot. Corns (thick, hardened layers of skin that develop when your skin tries to protect itself against friction and pressure) may develop on the bunion and/or on the neighboring toes. Bunions are more likely to occur in women.
Causes
- Heredity
- Wearing tight shoes that squeeze the toes together
- Arthritis
- Poor foot mechanics (the way your foot moves when walking)
A bunionette is a painful bump on the outside of the foot close to the little toe. It may develop a corn as well.
Diagnosis
It is diagnosed by your family doctor based on history, symptoms and a quick physical exam of your foot.
Treatment
Most patients do not need surgery. If your bunion is not painful, you do not need foot surgery. Surgery is NOT done for cosmetic reasons only.
Conservative treatment
- Wear shoes that are supportive and roomy (wide toe box) that do not put pressure on the bunion
- Shoes that fasten with laces or buckles give the feet more support than slip-ons
- Custom orthotics
- Toe spacers or bunion pads are also very useful
- NSAIDs (Advil/Ibuprofen) and/or pain relief (Tylenol/Acetaminophen) medication
Surgical Treatment
Surgical treatment is done to help with pain. There are several different surgical procedures to treat bunions. Each involves realigning the bones and soft tissues. The surgeon would discuss the specifics and risks of the recommended procedure.
While you go home the same day of surgery, the recovery can be long and painful. It can take 6 months to a year to fully recover.
If recovery of function after foot surgery proves to be challenging, you may choose to consult a physiotherapist who can help you recover your toe and foot movement, increase your foot, ankle and leg strength with exercise, and helping you restore a normal gait pattern.
Diabetic Foot/Charcot Foot
Diabetes is the result of the body’s inability to deal with elevated blood sugar, and it affects many people. Complications of diabetes can include poor blood circulation and nerve damage – both of which can affect the feet. Prevention of these problems is the key in diabetes treatment. Because nerve damage causes loss of feeling, the foot should be visually inspected daily for any new blister or small sore. These can progress quite quickly and become infected. If you notice any changes, please see your family doctor immediately for treatment.
Cause
Poor circulation can weaken bones and they can disintegrate or break. The advanced diabetic patient who suffers from diabetic peripheral neuropathy (altered or lost sensation in feet) will continue to walk on the foot because they cannot feel the pain from a broken bone. This can lead to more bones breaking and the sharp bone edges can damage and break the skin, causing ulcers to develop. The process of bone damage can lead to the foot becoming deformed – a condition which is called Charcot foot.
Symptoms
The person with Charcot foot may not have pain, but probably will have redness and swelling of the foot along with eventual deformity.
Diagnosis
Your family doctor may order an X-ray, MRI, or bone scan of the foot.
Treatment
Conservative treatmentThe goal of any treatment is to heal the broken bones and support foot deformities to prevent further damage. You may be treated with a cast or a boot for about 3 months in order to try to heal the bones. In this case, you will have weight-bearing restrictions, so the use of crutches or a walker or a wheelchair will be necessary. Once the swelling has decreased and the bones are fused together, you will likely need a special custom shoe.
Surgical treatmentSurgical treatment can involve shaving off extra bone, or fixing fractures with hardware (plates and screws), reconstructing and/or fusing joints in your foot. Usually patients will be casted and will have weight-bearing restrictions for a period of about 3 months.
Morton’s Neuroma
Morton’s Neuroma is a painful inflammation of a nerve in the ball of the foot. It involves a thickening of the tissue around one of the nerves in the foot. It usually occurs between the 3
rd and 4
th toe. It is often compared to the feeling of walking on a marble. Women are four times more likely to suffer from Morton’s Neuroma than men.
Causes
- Tight shoes (like high heels or cowboy boots)
- Prior injury to the foot that changes your foot mechanics
- Weak arch muscles leading to a flattening of the arch
- Heredity
Symptoms
Diagnosis
It is diagnosed ly your family doctor based on history, symptoms and a quick physical exam of your foot.
alTreatment
Conservative Treatment consists of:
- Roomy shoes with a soft sole with low heel
- Inserting a metatarsal pad in your shoe - to help lift and separate the bones in the forefoot and create less pressure in the tender area
- Icing or alternating ice and heat (2 min of each for a total of 16-20 minutes)
- NSAIDs (Advil/Ibuprofen) and/or pain relief (Tylenol/Acetaminophen) medication
- Custom orthotics (custom-made shoe inserts) might be considered
- Cortisone injection
- If your family doctor does not give cortisone injections, you may be referred to a sports medicine doctor
You may choose to consult a physiotherapist who will work with you to minimize swelling and pain, as well as help restore normal toe and foot movement as well as
muscle flexibility, function and strength.
Normally, 80% of patients have less pain with these measures.
Surgical treatment
Some people require foot surgery. Morton’s Neuroma excision is done by small incision on top of your foot. Following foot surgery, most recover in 6-8 weeks.
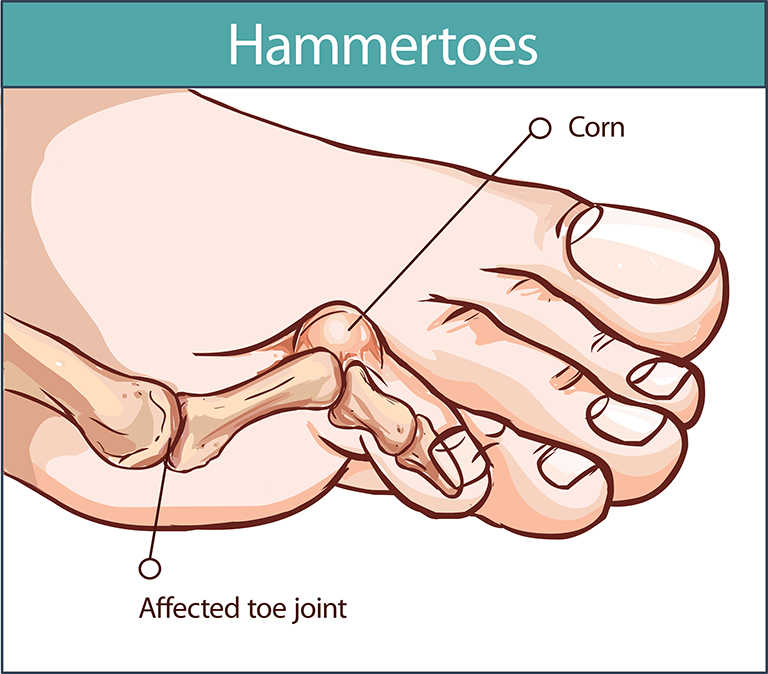 A hammer toe or claw toe is a deformity of the 2nd, 3rd, 4th or 5th toe where it bends at the middle joint to make it resemble a hammer or a claw. It makes the toe bend downward instead of pointing forward. This can cause problems because this abnormal toe position will put pressure on the toe when wearing shoes.
A hammer toe or claw toe is a deformity of the 2nd, 3rd, 4th or 5th toe where it bends at the middle joint to make it resemble a hammer or a claw. It makes the toe bend downward instead of pointing forward. This can cause problems because this abnormal toe position will put pressure on the toe when wearing shoes.
Generally, it is caused by a muscle imbalance in the foot. The deep (intrinsic) toe muscles on the top of the foot are weaker than the surface (extrinsic) muscles of the toes. It is commonly present with a bunion in the big toe. With time, it may become fixed in this position. Corns or calluses (thickened skin) may be present on the top of the bend in the toe. It can be painful.
Causes
- Muscle imbalance of the toe /foot muscles
- Ill-fitting shoes
- Poor foot mechanics
- Rheumatoid arthritis
- Prolonged period of not walking or weight-bearing (prolonged bedrest)
- Loss of feeling in toes (diabetic neuropathy)
- Prior injury to the toe
- High arches
Symptoms
- Pain in the toe when wearing shoes
- Corn and calluses (thick, hardened layers of skin that develop when your skin tries to protect itself against friction and pressure) on the toe, between the toes or on the ball of the foot
- Inflammation and redness of the toe
- Stiffening of the toe
Diagnosis
It is diagnosed by your family doctor based on history, symptoms and a quick physical exam of your foot.
Treatment
Conservative treatment
Hammer toes will progress slowly and may respond well to conservative treatment in the early stages. However, they require some intervention to prevent them from becoming progressively worse. Sometimes they progress rapidly and will eventually simply become fixed.
Conservative treatment involves:
- Roomy shoes with a broad toe box and a low heel (< 2”)
- Straps or splinting - to realign the toe
- Physiotherapy exercises to stretch and strengthen the muscles
- Toe cushions or non-medicated corn pads - to help protect the toe and make it more comfortable
- Orthotics (custom shoe inserts) may be recommended
Toe exercises should be done to stretch and strengthen the foot/toe muscles. You may seek help from a physiotherapist to guide you and show you how to exercise these muscles. It may also be necessary to stretch or strengthen in areas that may seem unrelated to your foot such as your hip, knee or core area. These are important in maintaining proper alignment and biomechanics through your leg onto your foot and toes.
Surgical treatment
In some cases, when the toe becomes rigid and painful or sores develop, foot surgery is needed. The type of surgery and recovery time will depend on your case.
Plantar Fasciitis
The plantar fascia is a fibrous structure under the skin on the bottom of the foot. It connects the heel to the front of your foot and supports your arch. This fascia can become inflamed and painful. With delayed healing or further injury, a calcium build-up can form on the heel bone. This is known as a heel spur. Plantar fasciitis can require a long time to heal (> 18 months).
Causes
Sometimes the cause cannot be identified as it often appears gradually for no apparent reason.
Some possible causes include:
- Tight calf muscles
- Very high or low arch
- Obesity
- New or increased activity and/or repetitive impact activity
- Prolonged standing on hard surfaces
- Poor footwear
- Weak foot/arch muscles
- Poor foot biomechanics
- Arthritis
- Poor circulation
Diagnosis
It is diagnosed by your family doctor based on history, symptoms, and a quick physical examination of your foot.
X-rays are not needed to confirm the diagnosis but may be necessary to rule-out other conditions when not responding to a trial of conservative treatment.
Symptoms
- Pain felt in the heel
- Worse after activity
- Painful first thing in the morning with the first steps
- Improves with activity as it warms up
- Pain may become constant
- Pain may be present at rest
Treatment
Conservative treatment
Over 90% of patients get better with conservative treatment, although the condition can take 6 to 18 months to resolve.
Conservative treatment consists of:
- Rest and/or activity modification
- Ice and heat contrasts (alternating 2 minutes of ice, 2 minutes of heat, for a total of 12 to 16 minutes)
- Massage
- NSAIDs (Advil/Ibuprofen) and/or pain relief (Tylenol/Acetaminophen)
- Over-the-counter or prescribed custom-made orthotics (shoe inserts)
- Supportive shoes which include a slight heel lift
- Physiotherapy
You may consult a physiotherapist who will guide you through techniques to decrease the pain as well as supervising a progression of exercises designed to improve your condition. Physiotherapy should consist of manual therapy (techniques to improve the joint mobility in your foot/ankle), massage, gentle stretching (keeping in mind that overstretching can perpetuate this condition), muscle strengthening exercises for your foot (possibly for your calf and leg too), and possibly foot taping. The physiotherapist might also look at your footwear, your gait and/or running technique. It typically takes 6-12 weeks for this condition to resolve with physiotherapy treatment.
Shockwave therapy might be suggested if conservative treatment has not been successful. TThe goal of shockwave therapy is to initiate a new healing process if the condition has become chronic.
Surgical treatment
Foot surgery is rarely considered and would depend on the patient’s presentation.
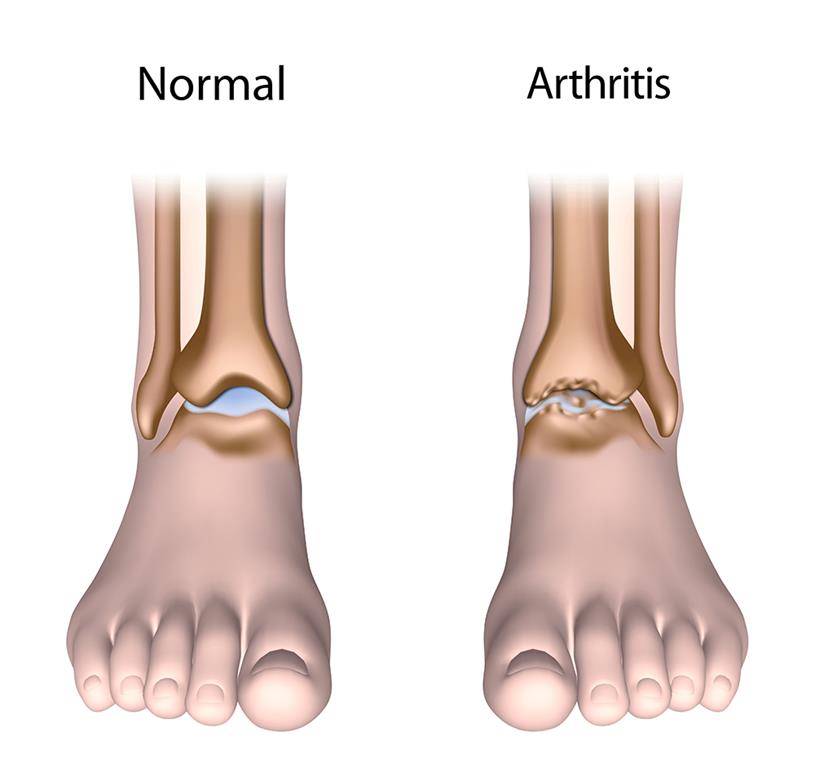 There are more than 100 types of arthritis that can affect the foot and ankle.
There are more than 100 types of arthritis that can affect the foot and ankle.
These are the 3 most common types:
Osteoarthritis: this is a degenerative or “wear and tear” kind of arthritis. Cartilage is a protective layer located between bones. Over time and with activity that cartilage wears down, until there is no longer any protection and bones rub against bones. Bone spurs (osteophytes) can be created. Pain and stiffness tend to increase over time. Risk factors for osteoarthritis include age, obesity and family history.
- Rheumatoid arthritis: this is a chronic disease that often begins in the foot and ankle on both sides of the body. It is an autoimmune disease, which means that the immune system attacks itself, resulting in swelling and pain in the joints. Eventually the joints are altered permanently.
- Post-traumatic arthritis: this can develop months or years after after an injury to the foot or ankle. It is similar to osteoarthritis as it is a “wear and tear” type of arthritis. It tends to develop years or months after an injury.
Symptoms
The symptoms will vary depending on the area of the foot affected.
Symptoms generally include:
- Ache at rest
- Pain with walking/weight-bearing
- Pain that flares up after an activity
- Tenderness in the affected area
- Joint swelling
- Warmth and redness
- Pain and swelling when getting up in the morning after sitting or resting for a long time.
Diagnosis
It is diagnosed by your family doctor based on history, symptoms, and a quick physical examination of your foot and ankle.
X-rays will confirm the diagnosis.
Treatment
Conservative treatment
Conservative management is always the first line of treatment.
This includes:
- Activity modification
- Exercises that minimize stress on the joints (swimming, biking)
- NSAIDs (Advil/Ibuprofen) and/or pain relief (Tylenol/Acetaminophen) medication
- Weight loss
- Supportive and comfortable footwear
- Walking aid (cane, walker, walking poles)
- Orthotics (custom insoles) or shoe inserts
- Physiotherapy
- Cortisone injection
- If your family doctor does not give cortisone injections, you may be referred to a sports medicine doctor
A physiotherapist can help manage the pain and introduce activities and exercises that encourage mobility and improvements in strength and function, as well as general fitness
Surgical treatment
Surgical management will depend on the joint affected and the severity of the arthritis, but can include:
- Cleaning out the arthritic joint
- Fusion of the joint to eliminate painful motion
- Replacing the joint
- After surgery, patients may need to wear a cast, braces or special shoes for a period of time. Recovery will depend on the procedure and the patient’s condition.
Achilles Tendinitis/Tear
The Achilles tendon is the largest tendon in the body. It connects the calf muscles to the heel and is working in almost every movement of the foot. Achilles tendinitis occurs when this tendon gets injured and inflamed from overuse, repetitive stress or degeneration. The tendon fibers can calcify at its attachment point on the heel bone and become hard with chronic tendinitis over time. Bone spurs (extra bone growth) can also develop in the tendon.
Achilles tendon rupture/tear
If you have experienced a sudden pain in the back of the leg or heard "pop" in the back of your calf or heel, you may have ruptured (torn) your Achilles tendon. This can happen without ever having any previous symptoms. Achilles tendon rupture is most commonly a traumatic sport injury that occurs in middle-aged men more than women. When it happens, you can usually still walk and move your ankle up and down, but you cannot come up on your toes on the injured leg. Go to Emergency or see your doctor immediately if you think you may have torn your Achilles tendon.
Causes
Achilles tendinitis is often caused by:
- Increase in activity levels
- Repetitive strain
- Inadequate training in a sport
- Poor footwear
- Tight calf muscles
- Problems with the shape/structure or function of the foot
- Weakness of the foot, calf or leg muscles
- Extra bone growth at the portion of the tendon that attaches to the heel bone.
Generally, tendinitis occurs when demands are more than the muscle is used to or can handle. The fibers of the tendon (the part of the muscle that anchors it to the bone) become inflamed and can break down. Tendinitis is also thought to originate from failed healing response.
Symptoms
- Gradual onset of aching, burning pain and stiffness in the heel
- Worse in the morning or after periods of rest
- Worse with exercise and the day after exercise.
- Swelling at the tendon attachment on the heel
- Warm and tender to touch at or above the heel bone
Diagnosis
Achilles tendinitis is diagnosed by your family doctor based on history, symptoms and a physical examination of your lower leg and foot.
An X-ray may be done to investigate whether you have a calcification on the heel or in the tendon, if your symptoms are chronic (lasting more than 6 months).
Treatment
Conservative treatmentThe recovery with conservative treatment for Achilles tendinitis can take from 3-6 months or longer. 90% of patients will get better with conservative treatment.
Treatment consists of:
- Activity modification - decrease in high-impact activities such as running and focus on low impact activities such as biking, swimming, elliptical exercise
- Icing (10-20 min applications as needed) or ice and heat contrasts (alternating 2 minutes of ice, 2 minutes of heat, for a total of 12 to 16 minutes)
- Oral (Advil/Ibuprofen) or topical (Emulgel) NSAID or pain relief (Tylenol/Acetaminophen) medication - However, recent research indicates the possibility that NSAIDs may slow down the healing process. You can discuss with your family physician.
- Gentle stretching - overstretching can perpetuate the problem
- Physiotherapy
- Heel lifts
- Supportive shoes
- Orthotics (custom insoles) or over-the-counter insoles
A physiotherapist can help you manage your pain symptoms and introduce gradual loading exercises to help the tendon heal. He/she will possibly also provide exercises to stretch and strengthen the other muscles in your legs, address core strength and motor control and look at your gait or running pattern.
Cortisone injections are controversial and typically not recommended, since they have been known to damage/rupture the tendon.
Shock wave therapy may be recommended for a slow healing tendon, since this treatment technique re-initiates the healing process.
Surgical treatment Surgical treatment is usually only considered if conservative treatment has proved ineffective for at least 6 months.
It involves cutting away the scar tissue and calcium deposits, and in some cases involves placing a tendon from elsewhere in the heel to assist the Achilles tendon.
After ankle surgery, patients usually wear a cast, boot or brace for a period of time and then need to do physiotherapy. Return to activity should be discussed with your surgeon. Therapy involving progressive exercises is necessary to recover your
maximum strength and function. Recovery can take 1-2 years.
Ankle Sprain/Ligament instability/Fracture

Ankle sprain is a very common injury. The most common type is the lateral ankle sprain (LAS) and it is caused by going over on the ankle with it pointed downward and twisted inward, injuring the ligaments on the outside of the ankle. It is common once you have sprained your ankle for it to happen again.
Symptoms
Depending on the seriousness of the sprain, symptoms are typically:
- Pain
- Swelling and bruising
- Difficulty putting weight on foot
- Pain with walking on the affected foot
If the ankle sprain is severe, and tearing of the ligaments occurs, it is possible that the injury will result in chronic instability of the ankle joint.
The symptoms of chronic ankle instability include:
- Persistent pain and swelling
- Recurrent ankle sprains
- Feeling like your ankle is “giving way”
- Decreased ability to return to activities and daily tasks for at least 12 months after the initial injury
Diagnosis
An ankle sprain is diagnosed by your family doctor based on history, symptoms and a physical examination of your foot and ankle.
Ankles sprains are graded 1 to 3, depending on how severely the ligament is injured.
Even though your ankle hurts, it doesn’t mean you need an X-Ray. Your doctor will choose to X-Ray your ankle only if the possibility of a fracture needs to be ruled out.
Treatment
Conservative treatment for an ankle sprain consists of:
- Icing
- Elevation – to help decrease swelling
- Crutches to walk – initially, to help decrease the weight placed on the injured ankle
- Ankle support or tensor bandage - for a short time
- Exercise
- Pain relief (Tylenol/Acetaminophen) medication or topical NSAID ( e.g.: Voltaren Emulgel)
- Physiotherapy
Early introduction of exercise and activity is encouraged to help speed up recovery.
Physiotherapy can provide education, a supervised exercise-based program that will focus on decreasing swelling, increasing your movement, strength, stability and balance. Recovery can take 6-12 weeks or longer.
Treatment for
chronic ankle instability consists of:
Wearing an ankle support for physical activity along with a comprehensive and progressive exercise program to improve your strength, motor control and balance, in order to prevent re-occurring sprains and return you to prior activity levels. A physiotherapist can help with this. Rehabilitation can take 3-6 months.
Ankle fracture
It is important to go to the Emergency Department of your nearest hospital or Urgent Care Centre if you are experiencing:
- Severe pain in the ankle
- Unable to stand or walk on your injured ankle
- If it appears out of place
If it is fractured, you will be put in an Aircast (removable cast) or a plaster cast, or you might require ankle surgery to repair the broken bones and fix them by installing plates and/or pins.
You likely will need to walk with crutches or a walker for approximately 6 weeks. This immobilization period will possibly need to be followed by some rehabilitation to restore your ankle mobility (mobilization and stretching), strength, balance, and proper walking pattern, before returning to full activity (such as stairs, sports, hobbies).